Exparel® provides long-lasting pain relief after surgery—up to 72 hours—helping patients recover more comfortably without the need for pain pumps.
Modern Pain Management
Exparel® delivers continuous pain relief through a single injection for up to 72 hours, eliminating bulky pain pumps and reducing reliance on opioids. Ideal for procedures like tummy tucks and breast augmentation.
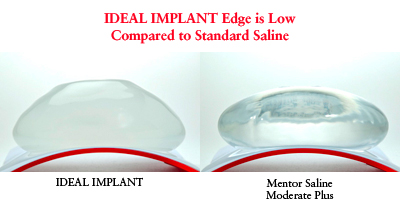
Natural feel is not the only thing women care about. The FDA approved intact silicone gel implants as safe. However, if a gel implant ruptures the implant and any gel should be removed including the surrounding capsule (capsulectomy). IDEAL® IMPLANT offers women natural feel without the risk of silent rupture. Women value the advantages of IDEAL® IMPLANT over silicone gel:
This is a very controversial topic with no clear answer. To my knowledge there is not a definitive study or consensus on this topic. Here is the background information: Breast implants (and other implantable medical devices) are widely believed to increase a patient’s risk of infection or capsular contracture from bacteria entering the blood stream (oral bacteremia) and settling on the implant causing an infection or capsular contracture. As dental treatment bacteremia is a rare cause of metastatic infections it makes it difficult to attribute causality.
Some surgeons treat their patients with prophylactic oral antibiotics in the period directly after breast augmentation with breast implants as well as for any procedure that causes transient bacteria, such as dental surgery, colonoscopy, urological procedures (e.g. cystoscopy), and gynecological procedures. Probably a single dose, one hour prior to the treatment followed by single dose after the treatment should be sufficient, as long as the patient is not immunocompromised.
Whether this should be done for the first 6 months to 1 year after the breast implant placement is unclear at best. To my knowledge, there isn’t any compelling data to support this. Intuitively many surgeons treat breast implants like other implantable medical devices like pacemakers and total joint replacements.
Even vaguer is dental cleaning. One could argue that we cause a bacteremia when we simply brush our teeth and so dental cleaning is only a more aggressive cleaning. Some surgeon’s recommendations may differentiate between superficial dental cleaning (no antibiotics) and deep cleaning and periodontal treatment (antibiotics therapy). There have been anecdotal reports of infection and capsular contracture following dental treatment. Therefore some plastic surgeons and patients after considering the risk of 1–2 doses of antibiotics vs the unlikely but potentially irreparable problems with your implant is worth the risk. As there is no great answer to this controversy, my recommendation is to follow the advice of your plastic surgeon and or other members of your health care team.
To understand why and how hair loss following surgery can occur, it is first necessary to understand the normal hair cycle. For example, everyone is constantly shedding hair (normal can be 100 scalp hairs shed per day) and this rate changes depending on many factors including surgery. Hair bulbs, the living part of hair, have three main phases: growth phase (anagen), involution/regressing phase (catagen), and the resting/quiescent phase (telogen). For the scalp the growth phase under normal conditions is 2-8 years, involution phase 2-3 weeks, and resting phase around 3 months. During times of stress such as surgery the majority of the hair can prematurely enter the rest phase, telogen, resulting in accelerated temporary hair loss. This is called telogen effluvium.
Stress and Hair Loss
Stress is a major factor in surgery-related hair loss. During stress our bodies shunt nutrients to our heart, lungs, muscles and other vital organs. As a result, hair may be weakened and in some cases, hair follicles stop producing new hair. This is called telogen effluvium. This is the most common form of hair loss and typically seen two to three months after a major body stress, such as major surgery, chronic illness, or significant infection. Other causes such as sudden change of hormone levels, especially in women after childbirth, or stopping hormone replacement. Hair may fall out from all parts of the scalp, and noticed on your pillow, shower/tub or on a hairbrush. Scalp hair may appear thinner, but it is unusual to see large bald spots. Unfortunately, all surgery involves some stress so it is important to minimize it to the extent possible. Suggestions like setting aside time in your day to both relax and exercise (walking in particular is a great stress reliever), taking part in calming activities all help. Educate yourself about your surgery and its recovery and discuss fears and concerns about your surgery with doctor, and try to focus on the final positive outcome.
Diet and Metabolism: During healing your body metabolism increases and there are increased needs for more nutrients such as protein, iron, zinc and biotin among others. Limited amounts will be diverted to wear it is needed the most with hair not being one of these places. To reduce the effects of stress on your hair, try to eat a more nutritious diet. Extra fruit and vegetables may help especially foods rich in zinc, biotin and (especially if a menstruating female) and iron. I recommend my patients take special perioperative vitamins made for this purpose as well as Arnica Montana and Bromelain to minimize inflammation.
Hormonal Changes and Hair Loss
Disruption to your normal hormonal cycle can result in hair loss. Though more pronounced in women but it can also affect men. Prolonged period of bed rest after surgery can affect this cycle, as can some of the drugs you may be given to help you heal after your operation. Limited exercise, such as walking frequently, is beneficial. Your doctor can let you know your limitations regarding exercise. It also helps to get back to eating in as regular a pattern as possible in the days after the surgery is complete.
Anesthesia and Hair Loss
It is inconclusive whether anesthesia causes hair loss, though both patients and many doctors believe there may be a link. If so, it is more likely with lengthy anesthetics periods lasting several hours rather than following shorter operations.
Limited research suggests that because anesthesia can slow down cell division, those cells which rely on fast cell division, such as hair follicles, are pushed into their resting phase. The good news is that this is temporary and the hair follicles will soon switch back to their normal irregular hair growth pattern. A large variety of things are associated with hair loss, including several diseases and hundreds of different drugs.
Field of surgery: Change of blood flow, and scarring (deep and at the skin level) can cause hair follicles to shut down restricting new hair growth. The current hair may go in the dormant phase (telogen) and fall out (telogen effluvium). Areas involved with scarring may result in areas of permanent loss of hair.
Medications: Literally hundreds of drugs may affect the growth of hair including some of which are necessary for surgical procedures. These can be direct effects or indirect effects (e.g. allergic reaction to a medication). Once the offending medication is stopped hair growth should slowly return to normal.
Other Factors: Other factors such as infection (bacterial, viral or fungal), scratching or too much pressure can result in hair loss after surgery (Positional Alopecia). All surgery represents an increased risk of infection. Once identified it needs to be treated quickly as can cause sudden hair loss. Positional Alopecia is uncommon, but can occur when the head is kept in one position for a prolonged time interval. This limits blood supply to the skin and hair follicles. Fortunately, when you sleep, you naturally move your head at intervals. This does not occur with surgeries that do not require or purposely restrict head movement. Typically this would apply to very lengthy surgeries lasting more than 6 hours.
The good news is that post-surgical hair loss doesn’t happen to most patients and, when it does, for most it comes back to normal within months.
If your asthma is optimally controlled the risk is very small and you can undergo major surgery without significant asthma complications. Most anesthesiologists I have worked with will recommend that you take your asthma medicine the prior to surgery with a sip of water and bring your inhalers to the surgery center. In addition, steroids are given just prior to anesthesia in most patients any way which helps prevent asthmatic complications.
On the other hand, if your asthma is poorly controlled, or you are steroid-dependent, you are at increased risk and therefore it is recommended that your asthma specialist provide any needed specific medical preparation prior to surgery including a written plan to give to your surgeon and anesthesiologist regarding asthma medication recommendations pre- and post-surgery. This will include a complete pre-surgical evaluation including pulmonary function test results, physical examination, and review of your medications and past medical problems. If your pulmonary function tests are not optimal your asthma doctor and/or anesthesiologist may choose to postpone surgery until your asthma is under optimal control prior to giving surgical clearance. In addition, it is advisable that you contact that anesthesiologist beforehand to discuss any issues that might arise and their management. . This is because surgery may cause an asthma flare or related bronchospasm during or immediately after surgery. Make sure you tell the anesthesiologist and your surgeon the amount and type of steroids you take so additional steroids can be given to prevent adrenal insufficiency which can result in a sudden blood pressure drop.
Diastasis Recti simply means a separation of the paired midline abdominal muscles also called the Rectus Abdominis muscles. Although not dangerous this condition makes your tummy stick out even if you have good core strength. Paradoxically with greater separation of these muscles, when you try to tense your muscles to tighten your tummy the center part bulges between the separated muscles. Here are some simple ways to determine if you have a significant Diastasis Recti: If you have a midline muscle gap of more than a few finger breadths when you contract your muscles and if you have bulging or protrusion in your midline between your muscles, especially if made worse when you contract your muscles. In my experience the vast majority of women after pregnancy have a Diastasis Recti, the same goes for massive weight gain/loss regardless of sex.
Repair of Diastasis Recti is typically done as part of a Tummy Tuck or Mommy Makeover procedure (regardless of technique) and consists of bringing the Rectus Abdominis muscles together by suturing (sewing) the inside edges of the muscle fascia together. I have found that it makes no difference if the suture material is absorbable or permanent, and typically I perform a two layer repair to insure that the correction is secure. Single layer closures may have a higher tendency of dehiscence (separation) that would require reoperation for repair. Although Diastasis Recti Repair can be done endoscopically for minor separations, this is no longer as popular of a procedure as there is a tendency for midline redundant skin unless there is wide undermining. Recovery is similar to most plastic surgical/muscle repair procedures: no heavy lifting or vigorous exercises for 4-6 weeks depending on your plastic surgeons wishes. With core exercises as part of your daily routine following this procedure you are well on your way to develop a “six pack Abs of Steel”.
Dr. Nichter’s tummy tuck patient, Michelle 45 years old, shares her story with the American Society of Plastic Surgeons (ASPS) about her plastic surgery journey.
Hitting newsstands today and Monday is an interesting article featuring Dr. Nichter and his patient, written by Joel Stein for Time Magazine, discussing the evolution of cosmetic surgery and it’s undeniable relevance in today’s world. The article titled “Nip. Tuck. Or Else” points out how thanks in part to social media we are now on the red carpet 24/7 posting pictures of ourselves on Facebook, Instagram, SnapChat, Vine, and more, so it’s imperative to look our best at all times. The social media frenzy is one reason why there has been a spike in the number of non-invasive procedures performed on the younger demographic. It can certainly be said that no longer are cosmetic procedures just for the aging population.
Here is the full article – Nip. Tuck. Or Else.”
by Joel Stein
You’re going to have to do it. And not all that long from now. Probably not a full-on, general-anesthesia bone shaving or muscle slicing.
But almost definitely some injections into your face. Very likely a session of fat melting in some areas and then possibly moving it to some other parts that could use plumping. Not because you hate yourself, fear aging or are vain. You’re going to get a cosmetic procedure for the same reason you wear makeup: because every other woman is.
No, it’s not fair that–in 2015, with a woman leading the race for the Democratic nomination for President–in addition to dieting, coloring your hair, applying makeup and working out, you now have to let some doctor push syringes in your cheeks just to look presentable. It’s not fair that you have to put your surgery on your credit card just so the other moms on the playground don’t overestimate your age. It’s not fair that you may risk your life going under general anesthesia just to keep up.
Then again, maybe it’s not fair that some women are born straight-nosed and full-breasted. That some people don’t have trouble staying thin. That workers with above-average looks will make $230,000 more over their lifetime than people who are in the aesthetic bottom seventh, as a study by University of Texas economics professor Daniel Hamermesh found. Maybe it doesn’t feel fair that a man is writing about this, even if more and more males are starting to feel the same kind of pressure that women have dealt with for decades.
“It’s becoming harder and harder to say no without being read as irrational or crazy,” says Abigail Brooks, the director of women’s studies at Providence College, who recently completed research comparing women who undergo antiaging interventions and those whom she calls “natural agers.” The former group described the latter using phrases like “let herself go” and “not taking good care of herself.” Brooks worries that that pressure is not only exhausting but also keeps women forever 21 emotionally. Continue reading “Dr. Larry Nichter featured in Time Magazine’s Article “Nip. Tuck. Or Else.””→
Dr. Larry Nichter, regarded as one of the top plastic surgeons in Southern California, talks about why he decided to specialize in the field of plastic surgery and about his humanitarian efforts made possible through his Mission Plasticos. To learn more about Plastics or to donate, please visit: http://www.themissionplasticos.org/
Dr. Nichter explains the risks and effects of smoking prior to and during recovery after plastic surgery. Smoking — specifically nicotine and carbon monoxide — impedes the body’s ability to deliver oxygen to tissues. As a result, the healing process after plastic surgery is negatively affected. Healing after plastic surgery has a significant effect on the quality of your result.
 Natural feel is not the only thing women care about. The FDA approved intact silicone gel implants as safe. However, if a gel implant ruptures the implant and any gel should be removed including the surrounding capsule (capsulectomy). IDEAL® IMPLANT offers women natural feel without the risk of silent rupture. Women value the advantages of IDEAL® IMPLANT over silicone gel:
Natural feel is not the only thing women care about. The FDA approved intact silicone gel implants as safe. However, if a gel implant ruptures the implant and any gel should be removed including the surrounding capsule (capsulectomy). IDEAL® IMPLANT offers women natural feel without the risk of silent rupture. Women value the advantages of IDEAL® IMPLANT over silicone gel:


